Autoimmune connective tissue disease of unknown etiology that affects the skin, blood vessels and internal organs.
Definition
- Sclerosis (histologic term)
- Homogenized, abnormally enlarged and eosinophilic collagen with a paucity of admixed fibroblasts (≠ fibrosis)
Etiologia: unkown
- Vascular dysregulation
- Immune dysregulation
- These abnormalities lead to the activation of fibroblasts and formation of fibrosis which characterizes the disease
Clinical presentation → classification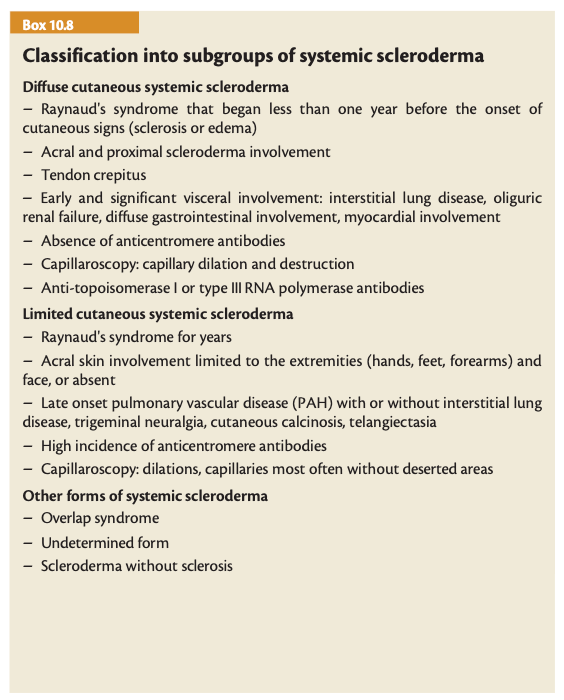
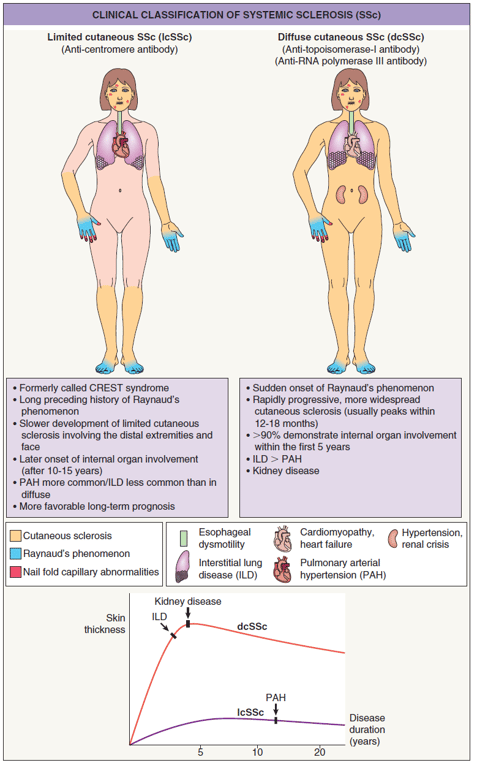
- Limited
- Includes CREST syndrome (because no all patients have all, “limited” term is favored)
- anti-Centromere antibodies
- Calcinosis cutis
- Raynaud’s syndrome
- Esophageal dysmotility
- Sclerodactily (sclerosis limited to fingers, hands and face)
- Early edema phase: may have digital pits
- Indurated phase
- Late atrophic phase (may lead to ulcers)
- Telangiectasias
- older patients and better survival than diffuse
- Systemic sclerosis sine scleroderma
- Abnormal nail fold capillaries
- Capillary loss (”drop-out”) alternating with dilated loops
- Sclerosis of the face
- Beaked nose
- Microstomia
- More youthful appearance
- Leukoderma of scleroderma
- Despygmentation with perifollicular sparing → “salt and pepper” sign
- Xerosis → pruritus
- May have pulmonary arterial hypertension
- Diffuse → early internal organ involvement (within 5 years), worse prognosis
- Raynaud’s syndrome
- Synovitis
- Tenosynovitis
- Tendon friction rubs
- Migratory polyarthritis
- Nail fold capillary dilation
- Esophagial dysfunction
- Pulmonary fibrosis
- Cardiac conduction defects
- Renal disease
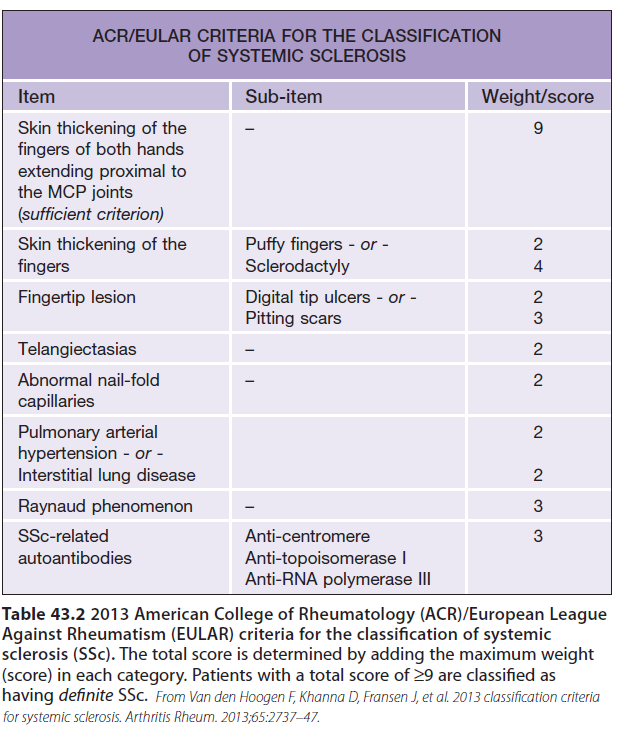
Diagnosis
- Classification criteria (for research) ≠ diagnostic criteria (may be broader)
- Major criteria: skin thickening proximal to metacarpophalangeal joints (9 points, automatic diagnosis)
- Minor criteria:
Exames complementares de diagnóstico
- Anticorpos
- ANA with nucleolar or discrete speckled (centromere) pattern → limited SS
- Topoisomerase I (Scl-70) → diffuse SS with pulmonary fibrosis
- anti-RNA polymerase III → diffuse SS with rapidly progressive skin disease and renal disease. Also increased risk of malignancy (mainly breast)
- Histology
Differential diagnosis
Tratamento
- Raynaud phenomenon
- Medidas gerais
- Manter mãos quentes, luvas
- Evitar tabaco
- Evitar roupa justa
- Evitar beta-bloqueantes e vasoconstritores nasais
- Vasodilatadores
- Calcium channel blockers
- Nifedipina 10mg PO 3x/dia
- Libertação prolongada - afalar
- Efeitos secundários: Headcahes, hot flashes, edema of lower limbs, GERD
- Amlodipina
- Nicardipine
- Diltiazem 2% cold cream QBP 50g
- Nitroglycerin ointment (diluted to 50% in petroleum jelly do reduce risk of headaches)
- Pentoxifilina 400mg 2id (trental)
- Alpha-blockers
- Prazozine
- Antiagregante plaquetário
- Ticlopidina 250mg
- Low-dose aspirin, clopidogrel
- Angiotensin II receptor blockers (eg. losartan 50mg id) may also be effective
- Endothelin receptor antagonists
- Bosentan 125mg 2id
- Parenteral prostaglandins
- ilomedin
- Phosphodiesterase type 5 inhibitors (eg. sildenafil, tadalafil)
- Risk: hypotension
- Fluoxetine 20mg id
- Botox injections
- Biofeedback
- Statins as vasoprotective effect
- Raynaud Phenomenon
- Cutaneous ulcers
- = Raynaud
- Oral Bosentan (oral endothelin receptor antagonist)
- IV iloprost (prostacyclin analogue)
- Treprostinil sc
- Nerve blocks and sympathectomies
- Cutaneous sclerosis
- ~Morphea
- D-penicillamine (historic, now rarely used)
- MTX if without Intersticial Lung Disease
- Mycophenolate Mophetil if Interstitial Lung Disease (2-3g id)
- Sirolimus
- Imatinib
- Calcinose cutis
- no effective medical therapy exists
- injeção intralesional com tiosulfato de sódio
- iboprost iv (perfusao lenta, precisa de internamento)
- diltiazem
- surgical excision
- Other: low dose warfarin, biphosphonates, probenecid, colchicine, TNF inhibitors, aluminium hydroxide, sodium thiosulfate, eletric shock wave lithotripsy
Na calcinose cútis pode se fazer injeção intralesional com tiosulfato de sódio ou fazer iboprost iv (perfusao lenta, precisa de internamento)
- Internal Organ Involvement
- ACE inhibitors for scleroderma renal crisis
- Cyclophosphamide (1-2mg/kg/dia)
- MMF
- Nintedanib for SSc-ILD
- Tocilizumab (IL-6 inhibitor)
- Pulmonary arterial hypertenstion
- Bosentan
- Phosphodiesterase type 5 inhibitors (sildenafil, tadalafil)
- Prostacyclin analogues: Iloprost (inhaled), epoprostenol (iv), treprostinil (inhaled, sc, iv)
- Oral prostacyclin receptor agonist selexipag
- Lung transplantation
- Other
- IVIg
- Rituximab
- autologous Hematopoietic Stem Cell Transplantation
 Made with Bullet
Made with Bullet